Trichotillomania
Hair-Pulling Disorder - Surgical Candidacy : Prioritizing behavioral health and psychological stability before surgical intervention.
What Is Trichotillomania?
Trichotillomania (often called "trich") is a mental health condition characterized by an irresistible urge to pull out one's own hair. It is classified as an Obsessive-Compulsive and Related Disorder.
What Are the Key Facts?
- Not a Weakness: It is a medical condition, not a character flaw or simple "bad habit."
- Prevalence: Affects approximately 1–2% of the population, often starting in childhood or adolescence.
- The Cycle: Typically involves a build-up of tension, the act of pulling, and a subsequent feeling of temporary relief or gratification.
- Treatable: Recovery is possible with appropriate psychological support and behavioral interventions.
How Is Trichotillomania Recognized?
Unlike genetic or autoimmune hair loss, trichotillomania presents with distinct physical signs caused by mechanical trauma.
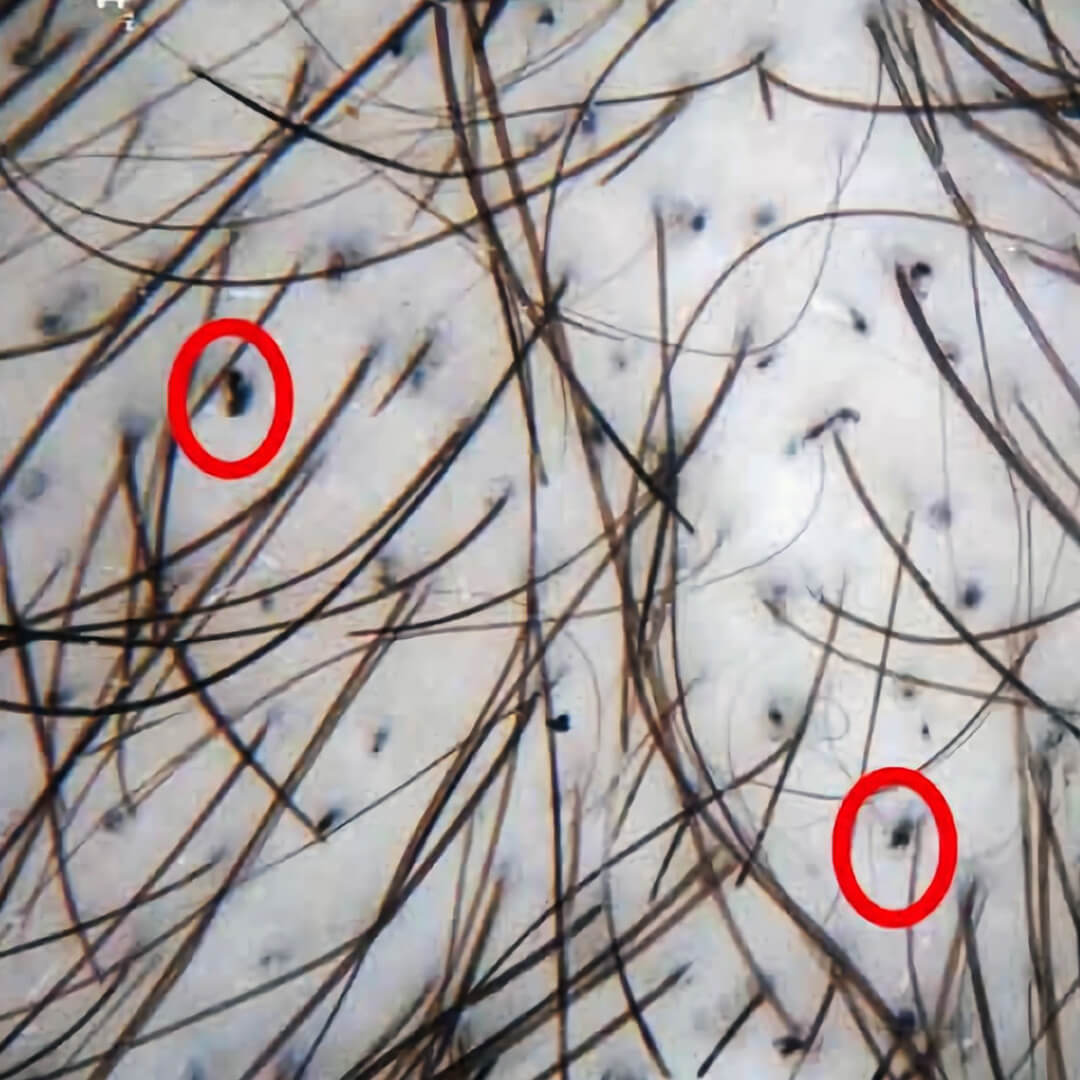
What Are the Clinical Signs?
- Irregular Patches: Bald spots often have strange, geometric, or straight edges rather than natural recession patterns.
- Variable Hair Lengths: The affected area contains hairs of many different lengths due to repeated breaking and regrowth.
- Broken Stubs: Presence of coiled strands, broken hairs, or dark stubs close to the scalp.
- No Scarring: Follicles are typically preserved (non-scarring), meaning hair can regrow if the pulling stops.
- Dominant Hand Pattern: Hair loss often occurs in areas easily reached by the dominant hand (e.g., a "Friar Tuck" pattern on the crown with sides intact).
What Is the Primary Treatment Path?
The first line of defense is always behavioral and psychological intervention. Surgery has no role until the underlying compulsion is fully managed.
Gold Standard: Behavioral Therapy
- Habit Reversal Training (HRT): Teaches individuals to recognize the urge to pull and replace it with a harmless competing action.
- Comprehensive Behavioral Model (ComB): Addresses sensory, cognitive, emotional, and environmental triggers to create a personalized management plan.
Supportive Medical Options
- N-Acetylcysteine (NAC): An over-the-counter amino acid supplement that has shown clinical promise in reducing the urge to pull.
- Medication: SSRIs or other psychiatric medications may be prescribed if anxiety, depression, or OCD co-exists, though therapy remains essential.
Recovery is a process of progress, not perfection. Self-compassion and professional support are critical components of success.
When Is Hair Transplant Considered?
Hair transplantation for trichotillomania is approached with extreme caution. It is never a cure for the disorder and carries a high risk of failure if the behavior persists.
Why Is Surgery High-Risk?
The compulsive urge does not distinguish between native hair and transplanted grafts. Pulling newly implanted follicles can destroy them permanently, leading to wasted resources, financial loss, and increased emotional distress.
When Is Surgery Contraindicated?
Surgery is strictly refused if:
- The patient has pulled hair within the past 12 months.
- Behavioral therapy has not been completed or engaged with.
- A mental health provider has not cleared the patient for surgery.
- Expectations are unrealistic (e.g., believing surgery will stop the urge).
What Are the Strict Criteria for Consideration?
Surgery might only be discussed as a last resort for permanent cosmetic repair if ALL of the following are met:
- Long-Term Stability: Documented zero pulling for a minimum of 12–24 months, verified by self-report and a support person or therapist.
- Therapy Completion: Successful completion of a structured behavioral therapy program (e.g., HRT).
- Psychiatric Clearance: Written support from a psychiatrist or psychologist confirming stability and assessing low relapse risk.
- Informed Consent: Full understanding that relapse could destroy the grafts and that surgery does not address the underlying psychological condition.
Even when these criteria are met, risks remain elevated. Post-operative itching, stress, or life changes can reactivate the urge to pull.
Key Takeaways
- Trichotillomania is a recognized mental health condition (OCD-related), not a structural hair loss or a "bad habit."
- Surgery is contraindicated during active pulling. Transplanted grafts are just as vulnerable to being pulled out as natural hair.
- Behavioral Therapy First: Habit Reversal Training (HRT) and psychological support are the primary and most effective treatments.
- Strict Candidacy: Surgery is only considered after 12–24 months of documented stability and written mental health clearance.
- High Risk of Relapse: Even with stability, post-operative stress or itching can trigger the urge again, potentially destroying the results.